
Abstract
Purpose: To describe the frequency and pattern of drug errors in clinical anesthesia, and to evaluate whether a change to colour coded syringe labels, along with education, could reduce the problem of drug errors.
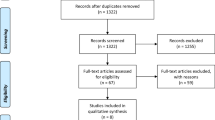
Methods: We prospectively recorded anesthesia-related information from all anesthetic cases for 36 mo, totally 55,426 procedures. Intraoperative problems, including drug errors, were recorded. After eighteen months we changed to colour coded syringe labels, and the effect of this change and education on drug errors was assessed. Errors were divided into four groups: syringe swap, ampoule swap, other ‘wrong drug’ errors, and wrong dose errors. The problems were graded into four levels, according to severity.
Results: A drug error was recorded in 63 cases (0.11%). There were 28 syringe swaps, and muscle relaxants were erroneously given in 15. There were nine ampoule swaps. There were eight ‘other wrong drug’ cases, and 18 cases where a wrong dose of the correct drug was given. Three of the drug errors were classified as serious, and 27 were of moderate severity. We found no differences between the two periods except for decreased number of ampoule swaps (P=0.04).
Conclusion: Drug errors are uncommon, and represent a small part of anesthesia problems but still have the potential for serious morbidity. Syringe swaps occurred most often between syringes of equal size, and were not eliminated by colour coding of labels. As muscle relaxant drugs are most commonly involved, and can cause lasting morbidity, special preventive measures should be taken for this group of drugs.
Résumé
Objectif: Décrire les erreurs de médicaments en anesthésie clinique selon leur fréquence et leur nature et évaluer si une modification de la couleur des étiquettes codées des seringues pouvait, avec une certaine formation, résoudre ce problème.
Méthode: On a enregistré, lors d’une étude prospective, les informations reliées à tous les cas d’anesthésie, 55 426, pendant 36 ms. ainsi que les problèmes peropératoires, y compris les erreurs de médicaments. Après 18 ms, on a introduit des étiquettes de couleur codées et évalué l’effet de ce changement et de l’information donnée sur les erreurs de médicaments. On a divisé les erreurs en quatre catégories: échange de seringue, échange d’ampoule, autre «médicament incorrect» et erreurs de doses, et classé les problèmes selon quatre niveaux de sévérité.
Résultats: Il y a eu 63 cas d’erreurs de médicaments (0,11 %). On a noté 28 échanges de seringues et 15 cas ontreçu des myorelaxants par erreur. De plus, 9 échanges d’ampoules ont eu lieu, 7 cas d’«autres médicaments incorrects» et 18 cas d’erreurs de doses pour le médicament requis. Parmi ces erreurs, 3 étaient sévères et 37 étaient modérées. Il n’y a pas eu de différence entre les deux périodes, sauf en ce qui concerne la baisse d’échanges d’ampoules (P=0,04).
Conclusion: Les erreurs de médicaments sont rares et ne représentent qu’une petite partie des problèmes anesthésiques, mais elles sont toujours potentiellement dangereuses. Les échanges de seringues surviennent le plus souvent entre seringues de même taille et ils ne sont pas réduits par les étiquettes de couleurs codées. Les myorelaxants, le plus souvent en cause, peuvent entraîner une morbidité résiduelle. Des mesures préventives spéciales devaient être envisagées dans ce cas.
Article PDF
Similar content being viewed by others


References
Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med 1991; 324: 377–84.
Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential drug events. JAMA 1995; 274: 29–34.
Bates DW, Boyle DL, Vander Vliet MB, Schneider J, Leape L. Relationship between medication errors and adverse drug events. J Gen Intern Med 1995; 10: 199–205.
Phillips DP, Christenfeld N, Glynn LM. Increase in US medication-error deaths between 1983 and 1993. Lancet 1998; 351: 643–4.
Cohen MM, Duncan PG, Pope WDB, et al. The Canadian four-centre study of anaesthetic outcomes: II. Can outcomes be used to assess the quality of anaesthesia care? Can J Anaesth 1992; 39: 430–9.
Currie M, Mackay P, Morgan C, et al. The “wrong drug” problem in anaesthesia: an analysis of 2000 incident reports. Anaesth Intensive Care 1993; 21: 596–601.
Chopra V, Bovill JG, Spierdijk J. Accidents, near accidents and complications during anaesthesia. A retrospective analysis of a 10-year period in a teaching hospital. Anaesthesia 1990; 45: 3–6.
Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection. Anesthesiology 1984; 60: 34–42.
Cullen DJ, Bates DW, Small SD, Cooper JB, Nemeskal AR, Leape LL. The incident reporting system does not detect adverse drug events: a problem for quality improvement. Jt Comm J Qual Improv 1995; 21: 541–8.
Sanborn KV, Castro J, Kuroda M, Thys DM. Detection of intraoperative incidents by electronic scanning of computerized anesthesia records. Comparison with voluntary reporting. Anesthesiology 1996; 85: 977–87.
Jayasuriya JP, Anandaciva S. Compliance with an incident report scheme in anaesthesia. Anaesthesia 1995; 50: 846–9.
Currie M. A prospective survey of anaesthetic critical events in a teaching hospital. Anaesth Intensive Care 1989; 17: 403–11.
Leape LL. Error in medicine. JAMA 1994; 272: 1851–7.
Williamson JA, Webb RK, Sellen A, Runciman WB, Van der Walt JH. Human failure: an analysis of 2000 incident reports. Anaesth Intensive Care 1993; 21: 678–83.
Leape LL, Bates DW, Cullen DJ, et al. Systems analysis of adverse drug events. JAMA 1995; 274: 35–43.
Davies JM, Webb RK. Adverse events in anaesthesia: the wrong drug (Editorial). Can J Anaesth 1994; 41: 83–6.
Orser BA, Oxorn DC. An anaesthetic drug error: minimizing the risk. Can J Anaesth 1994; 41: 120–4.
Heneghan CPH. Drug labelling — a place for colour coding? Anaesthesia 1996; 51: 600–12.
Merry AF, Webster CS. Labelling and drug administration error (Letter). Anaesthesia 1996; 51: 987–8.
Nunn DS, Baird WL. Ampoule labelling (Editorial). Anaesthesia 1996; 51: 1–2.
Fasting S, Gisvold SE. Data recording of problems during anaesthesia: presentation of a well-functioning and simple system. Acta Anaesthesiol Scand 1996; 40: 1173–83.
Cooper JB. Is voluntary reporting of critical events effective for quality assurance? (Editorial). Anesthesiology 1996; 85: 961–4.
Rosner B. Fundamentals of Biostatistics, 5th ed. Pacific Grove, CA: Duxbury, 2000: 386.
Cohen MM, Duncan PG, Pope WDB, Wolkenstein C. A survey of 112,000 anaesthetics at one teaching hospital (1975–83). Can Anaesth Soc J 1986; 33: 22–31.
Spittal MJ, Findlay GP, Spencer I. A prospective analysis of critical incidents attributable to anaesthesia. Int J Qual Health Care 1995; 7: 363–71.
Heier T, Steen PA. Awareness in anaesthesia: incidence, consequences and prevention. Acta Anaesthesiol Scand 1996; 40: 1073–86.
Moerman N, Bonke B, Oosting J. Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology 1993; 79: 454–64.
Short TG, O’Regan A, Jayasuriya JP, Rowbottom M, Buckley TA, Oh TE. Improvements in anaesthetic care resulting from a critical incident reporting programme. Anaesthesia 1996; 51: 615–21.
Ouchterlony J, Arvidsson S, Sjöstedt L, Svärdsudd K. Peroperative and immediate postoperative adverse events in patients undergoing elective general and orthopaedic surgery. The Gothenburg study of perioperative risk (PROPER). Part II. Acta Anaesthesiol Scand 1995; 39: 643–52.
Junger A, Veit C, Kloss T. Four year’s experience with quality assurance in anesthesiology in Hamburg. (German) Anasthesiol Intensivmed Notfallmed Schmerzther 1998; 33: 417–24.
Junger A, Veit C, Kloss T. Continuous improvement in anesthesiological quality documentation. (German) Anasthesiol Intensivmed Notfallmed Schmerzther 1998; 33: 715–21.
Bates DW. Medication errors. How common are they and what can be done to prevent them? Drug Saf 1996; 15: 303–10.
Runciman WB, Sellen A, Webb RK, et al. Errors, incidents and accidents in anaesthetic practice. Anaesth Intensive Care 1993; 21: 506–19.
Allnutt MF. Human factors in accidents. Br J Anaesth 1987; 59: 856–64.
Radhakrishna S. Syringe labels in anaesthetic induction rooms. Anaesthesia 1999; 54: 963–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fasting, S., Gisvold, S.E. Adverse drug errors in anesthesia, and the impact of coloured syringe labels. Can J Anaesth 47, 1060–1067 (2000). https://doi.org/10.1007/BF03027956
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03027956